DO NOT USE - ALL INFORMATION LIKELY INCORRECT IF NOT ACTIVELY DANGEROUS
Please use current guidelines available on the UHNM intranet for patient treatment
Please use current guidelines available on the UHNM intranet for patient treatment
RECOGNITION AND ASSESSMENT
- Falls are common in the elderly
- may be the presenting symptom of an acute illness
- Causes are generally multifactorial
Falls and syncope
- Often overlap or difficult to distinguish
- patient may have no memory of the event
- may be no eyewitness accounts
- See blackout/syncope guideline
Risk factors
- Gait and balance impairment
- Reduced muscle strength
- Reduced visual acuity
- Cognitive impairment
- Drugs - polypharmacy
- sedatives/hypnotics, antidepressants, neuroleptics
- diuretics, class 1 anti-arrhythmics, alcohol, anti-cholinergics
- Predisposing conditions
- alzheimer’s disease, stroke, Parkinsonism,
- depression, visual impairment
- peripheral neuropathy, arthropathy, cardiac failure
- Environmental hazards
- poor lighting, loose carpets, lack of safety equipment
- poorly fitting shoes or clothes
History
Circumstances of fall
- Obtain an eye witness account if possible
- Ask for information that may suggest:
- syncope
- vertigo
- dizziness
- unsteadiness
- seizures
Consequences of the fall
- Time spent on floor
- Injuries sustained
Document any risk factors
- Medications that can precipitate postural hypotension
- History of falls, including previous fractures
- Impaired mobility
- Fear of falling
- Poor vision
- Incontinent of urine
- Confirmed dementia
Social history
- Carer support
- Lives alone?
- Environmental hazards
Examination
Cardiovascular
- Check for postural drop (after standing for 3 min)
- 20 mmHg in systolic BP or 10 mmHg in diastolic BP
- if drop confirmed, review diuretic therapy, antihypertensives and major tranquillizers
- Arrhythmias
- Structural heart disease
- Heart failure
Neurological
- Evidence of head injury
- Glasgow Coma Score
- Vision
- Muscle strength
- Tone
- Lower extremity peripheral nerves
- Proprioception
- Extrapyramidal and cerebellar function
Cognitive assessment
- Complete a 4AT score first to screen for both delirium and/or dementia, then
- Once confusion lessens complete a Six item cognitiveimpairment test (6 CIT) score to assess for cognitive impairment
Locomotor
- Evidence of hip fracture or other bony injury
- Presence of muscle wasting
- Leg ulcers
- Deformities
INVESTIGATIONS
- FBC, U&E
- ECG
- Urinalysis
- Imaging to identify injuries or acute illness
RISK ASSESSMENT
A&E
- Check the Patient Risk Assessment completed by A&E nursing staff
Falls in hospital
- Complete post falls proforma and a STOP5 debrief
- ensure all interventions required have taken place
IMMEDIATE MANAGEMENT
- Treat injuries
Acute medical problems
- Commence treatment and refer to appropriate medical team
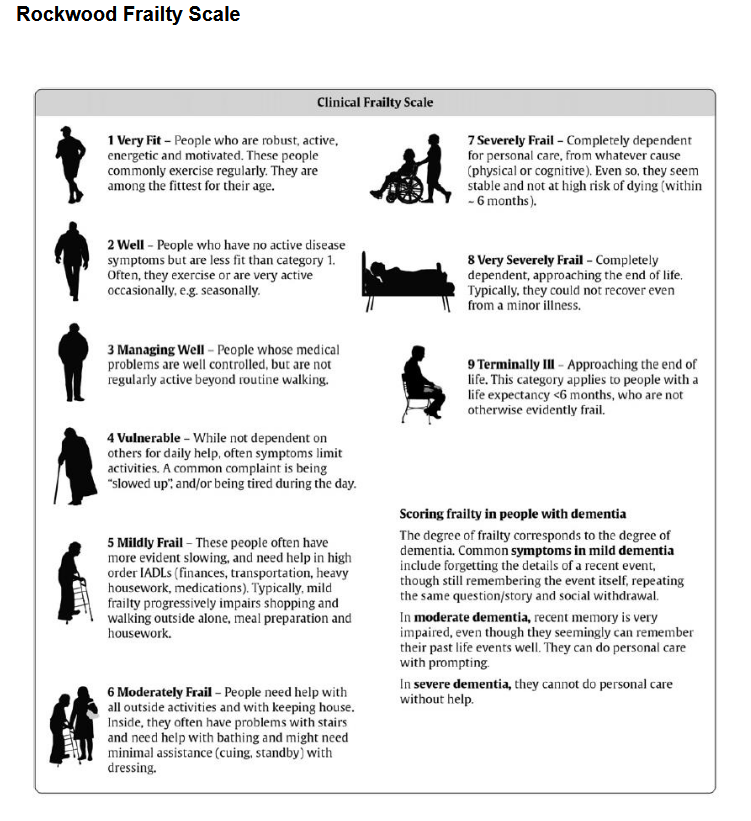
- If patient has Rockwood Clinical Frailty Score of ≥4 and requires admission, request elderly care bed
- If syncope suspected, see blackout/syncope guideline
SUBSEQUENT MANAGEMENT
- Ward nursing staff complete Patient Risk Assessment booklet
- Start falls prevention care plan with a list of interventions
- In plan, doctor/pharmacist complete a medication review
- assess stopping/reducing drugs e.g. antidepressants, night sedation, antipsychotics, and antihypertensives
Full multifactorial assessment
Drugs
- Check medications that may cause falls
- Polypharmacy, especially if:
- cardiovascular drugs
- insulin or oral hypoglycaemic agents
- hypnotics
- psychotropic drugs
- Alcohol
Environment
- Refer to occupational therapy
Neurovascular problems
- Gait and balance, refer to physiotherapy
Living arrangements
- Social work referral
Investigations
Cardiovascular
- If aortic stenosis or hypertrophic obstructive cardiomyopathy (HOCM) suspected, echocardiogram
- 24 hr tape if:
- bradycardia
- first degree atrioventricular block
- right bundle branch block (RBBB) and left axis deviation
- second or third degree atrioventricular block
- recurrent episode of loss of consciousness, with no features of epilepsy
- if abnormalities on 24 hr tape, cardiology referral may be needed
Neurological
- If epilepsy suspected, EEG
- if EEG suggestive of epilepsy, see First seizure guideline
Osteoporosis Assessment
- Check for a history of fragility fracture (wrist, spine, hip, pelvis or neck of humerus)
- Vertebral fractures are common and often missed
- check imaging for any vertebral wedging/height loss/collapse
- if back pain, kyphosis, or height loss >2 inches, consider x-ray thoracic and lumbar spine
Previous fragility fracture
- Refer to Fracture Liaison Service
- For any patient not taking a bisphosphonate, check if it is contraindicated or tried and not tolerated
- If no contraindication and no report of intolerance, prescribe an oral bisphosphonate alendronate 70 mg or risedronate 35 mg once per week on the same day, swallowed whole ≥30 min before first food, beverage, or medicinal product of the day with plain water only. Patients should not lie down for ≥30 min after taking alendronate or risedronate
- prescribe concomitant daily calcium and vitamin D supplementation, to be taken ≥30 min after bisphosphonate on the day this is also taken
- If fracture spontaneous, check bone profile, thyroid function, and consider myeloma screen
No history of fragility fracture
- Check bone profile and consider Calcium and Vitamin D supplementation
- Use FRAX, remember to enter UK and if Bone Mass Density (BMD not available, leave blank) to determine future fracture risk and need for further treatment or DXA scan
- if at intermediate risk (yellow) in FRAX, refer for DXA scan
- if at high risk of fracture in FRAX, consider an oral bisphosphonate, or if intolerant/unsuitable, refer to osteoporosis service
Specialist referral
- Depending on clinical findings, refer to appropriate specialist
Recurrent falls
- Unless patient has moderate-severe dementia, refer to Falls service
DISCHARGE
- If at high risk of falls (a YES answer to any of the 4 falls risk screening questions in Patient Risk Assessment booklet) explain in discharge letter
- If medical team feel further outpatient investigation or attendance at a Falls programme required, refer patient to Falls service
- information about recent falls and falls-related injuries
- known contributing factors (medical history etc.)
- If inpatient echo and 24 hr tape have been requested, doctor who ordered the test to forward the results to the GP
Last reviewed: 2024-03-14