DO NOT USE - ALL INFORMATION LIKELY INCORRECT IF NOT ACTIVELY DANGEROUS
Please use current guidelines available on the UHNM intranet for patient treatment
Please use current guidelines available on the UHNM intranet for patient treatment
- Actively manage patients with ≥2 capillary glucose levels >12 mmol/L in 24 hr
- Refer patients with persistent hyperglycaemia (>12 mmol/L), DKA or HHS to diabetes team
- for full list of criteria for referral to diabetes team, see referral to diabetes team guideline
RECOGNITION AND ASSESSMENT
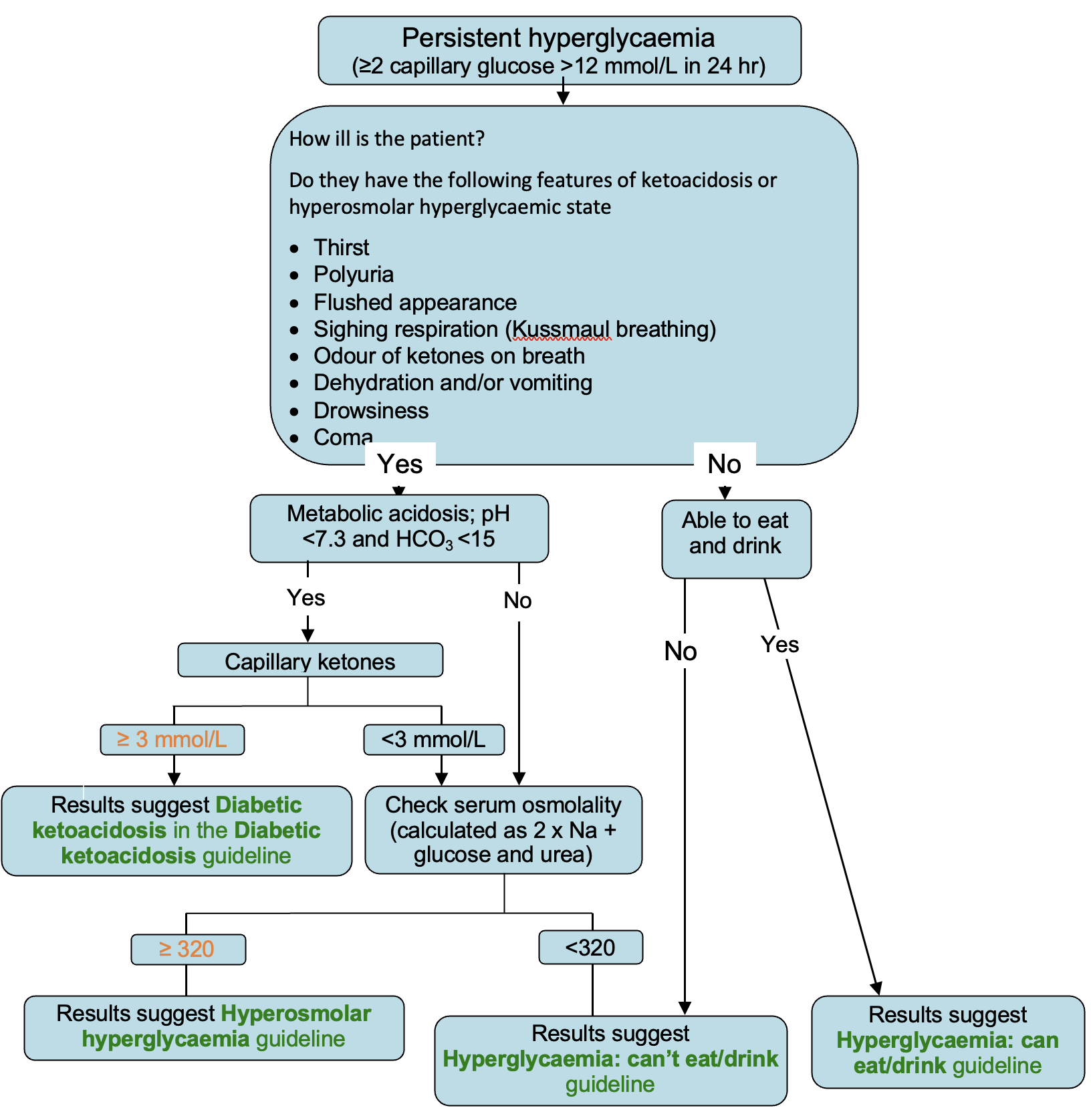
Symptoms and signs suggesting DKA or HHS
- Thirst
- Polyuria
- Flushed appearance
- Hyperventilation (Kussmaul breathing)
- Odour of ketones on breath – not always present or detectable
- Dehydration and/or vomiting
- Drowsiness
- Coma
Investigations for classifying hyperglycaemia
- Blood glucose (capillary)
- Test for ketones in urine
- U&E
- Blood glucose (venous)
- Venous blood gases
- if SpO2 <94%, arterial blood gas
- If metabolic acidosis present (pH <7.3), check capillary (blood) ketones
- if not available on ward, assume acidosis with high glucose and ketonuria is DKA unless proved otherwise
- even in type 2 diabetes, severe hyperglycaemia can temporarily suppress insulin secretion leading to keto (metabolic) acidosis
- however, in any metabolic acidosis, check for causes other than diabetic ketoacidosis
- Calculate or measure serum osmolality (2 x Na + urea + glucose)
Last reviewed: 2023-10-23