DO NOT USE - ALL INFORMATION LIKELY INCORRECT IF NOT ACTIVELY DANGEROUS
Please use current guidelines available on the UHNM intranet for patient treatment
Please use current guidelines available on the UHNM intranet for patient treatment
In hyperkalaemia in a dialysis patient, contact renal team urgently for advice
In patients with DKA, follow Diabetic ketoacidosis guideline
In patients with DKA, follow Diabetic ketoacidosis guideline
RECOGNITION AND ASSESSMENT
- ABCDE approach and NEWS system
- Comprehensive medical and drug history and clinical examination to determine the cause of hyperkalaemia
Symptoms and signs
- Frequently none, or non-specific neuromuscular symptoms
- Muscular weakness may occur if blood K+ >7.0 mmol/L
- Cardiac arrest without warning
- ECG changes (see Treatment)
Investigations
- In emergency, measure K+ on a point-of-care blood gas analyser and initiate treatment whilst awaiting the results from a laboratory plasma sample (green top; lithium heparin)
- HCO3- in venous blood (or from blood gases, if indicated for other reasons) and lactate
- If serum K+ ≥6.0, urgent 12-lead ECG. If ECG abnormal, or rapid rise in K+ levels and in patients with plasma K+ ≥6.5 mmol/L, continuous 3 lead cardiac monitoring; ideally in a high-dependency setting
Common Causes
- Artefact: release from blood cells (e.g. during clotting, blood dyscrasias, haemolysis, delayed centrifugation of sample for >2 hr)
- Low molecular weight heparin
- Failure of excretion: renal failure, mineralocorticoid deficiency, drugs e.g. spironolactone, amiloride (potassium sparing diuretics), ACE inhibitors (~prils), angiotensin II blockers (~sartans), aliskiren, NSAIDs, ciclosporin, tacrolimus
- Release from cell: severe tissue damage, acidosis (consider DKA, lactic acidosis)
- Excess ingestion or supplementation
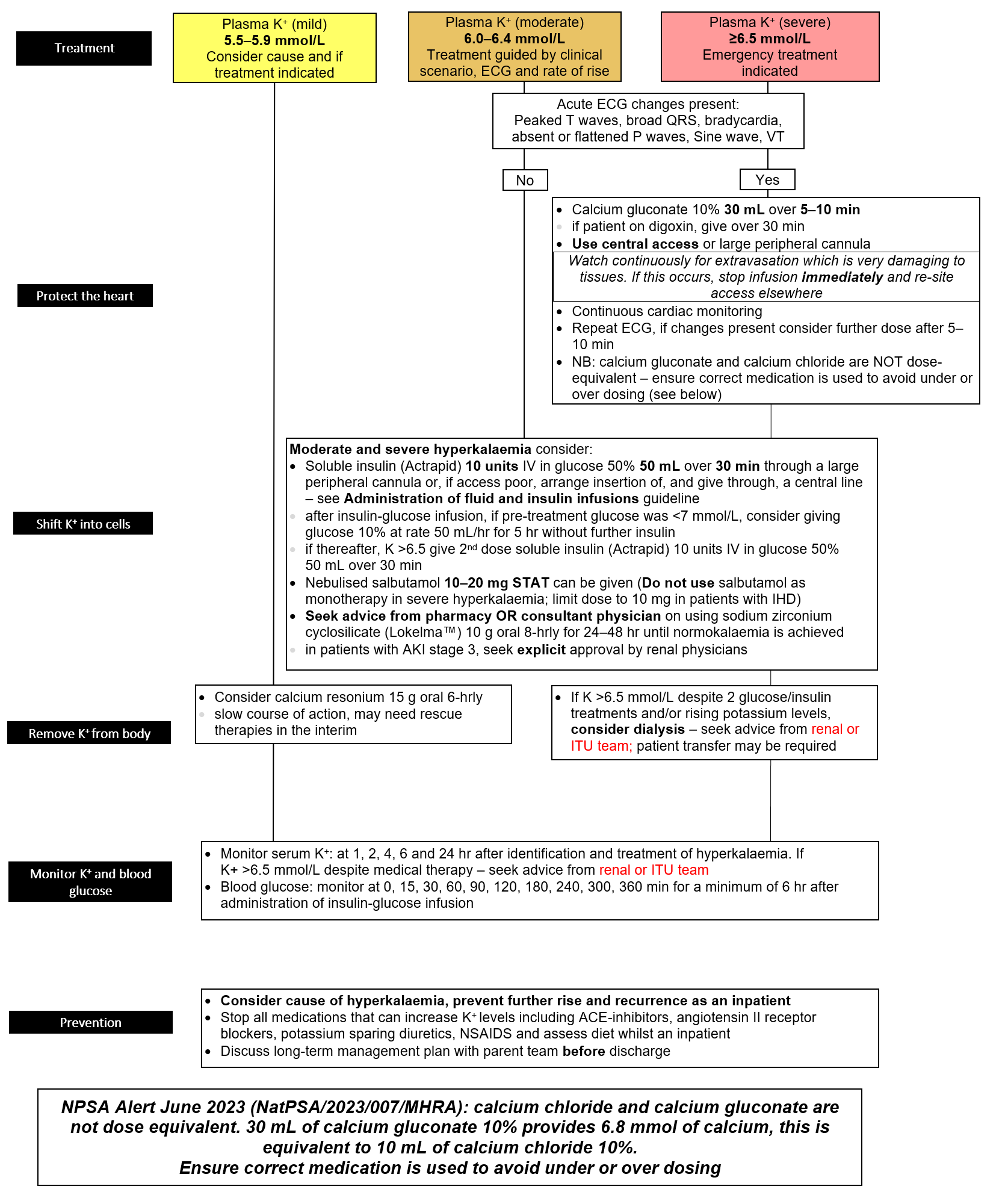
MANAGEMENT
- If refractory shock/other organ failure or cause not known, seek advice from ITU and or renal team
- Protect the heart and lower K+. For guidance follow algorithm below
- Treat the underlying cause
Last reviewed: 2024-02-19